
Join our Team of Volunteers!
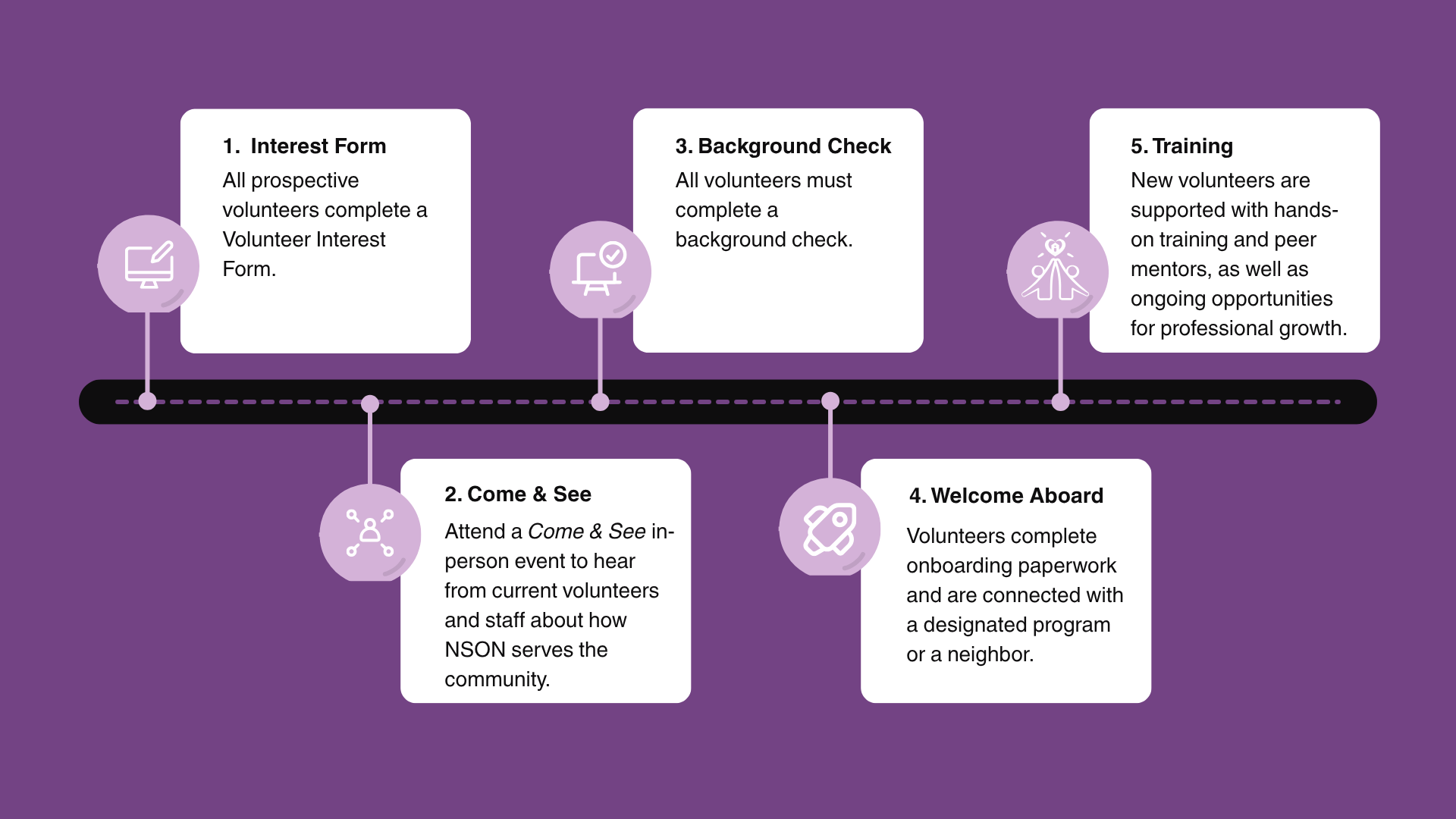
Prospective Volunteer Roadmap
Volunteers are the heart of Nurses Serving Our Neighbors, making our work and growth possible every day.
We welcome both medical and non-medical volunteers to join us in serving our community.
Our volunteers are licensed nurses, case managers, interpreters, prayer warriors, and others with a passion for helping our neighbors achieve their health goals.
Note: We ask for a commitment of at least 1 year from the time of onboarding.
“NSON has been more than a volunteer opportunity. It has allowed me to serve others while showing and sharing the love of God. I leave every event with my heart full from not only the neighbors we serve but also my peers. The love and care is genuine and it feels good to make a difference in the community with people that you truly care about and that care about you.”
“That’s what I love about NSON. I feel like I can care for the whole person.”
“Invariably, I come away with more than I can ever give.”